
Critical Decisions in Critical Moments: Goals of Care in the Critical Care Setting
Authors: Rhea Bhargava, DO PGY2, Bianca Persaud, MD PGY2, Anna Braendle, MD PGY2
Peer Reviewer: Amy Hembree, MD PGY3, Lauren Gruffi, MD PGY3
Faculty Editor: Bruce Gutierrez, DO, Emergency Medicine and Palliative Medicine
Introduction
We hear the overhead announcement: “85 year old female in cardiac arrest coming back to DART Room.” Our team immediately rushes into the DART room to set up for ACLS and all of the invasive procedures this patient may require for resuscitation - intubation, central line, arterial line, etc. The team notices a family member—her son—standing quietly in the corner, visibly anxious and unsure whether to speak as we move quickly into action. In the urgency of the moment, it’s easy to overlook him, but perhaps we should pause - what if he doesn't want us to perform chest compressions and potentially break her frail ribs? What if she wouldn't want to have a breathing tube and be stuck on a ventilator for the rest of her life? ? What if we decided to focus on patient comfort instead of maximally invasive measures?
Goals of care conversations are defined as a discussion centered on medical treatment that aligns with the patient's values, preferences, and priorities, supporting patient autonomy and promoting patient-centered care. We can all agree that goals of care (GOC) discussions are vital to providing care, especially in the ED. However, in the hustle and chaos of our environment, we may not feel like there is time for a GOC conversation, or may not feel comfortable doing so, and ultimately defer the conversation to our colleagues upstairs. Particularly in the setting of trauma or critical care, we tend to assume that doing “the most” is warranted. However, this may not always be the case, and it is important we take this into consideration. We have a unique role in the ED, as we are the first few people to meet a patient and their loved ones on what could be the worst day of their lives. This is a unique opportunity but also poses its challenges - our time with patients can be as short as hours or even minutes, but during that time a patient’s clinical status can change drastically, and major medical decisions may need to be made. How do we ensure that we’re providing goal concordant care? Whose job is it to have the conversation? Do we wait for the inpatient team? When is the right time?
Why We Care about GOC
A 2012 study of Medicare patients participating in a longitudinal study from 1992 to 2006 found that 75 percent of decedents presented to the emergency department within the final six months of life [2]. However, 55 to 100 percent of older adults present without advanced directives [3]. Taken together, these findings suggest that many patients who are either seriously ill, or will soon become seriously ill, pass through the emergency department, and that the majority of these patients do not have clearly documented GOC. Without this knowledge, we run the risk of potentially harming the patient–providing intense, invasive, often painful care at the end of life.
Goals of care conversations have been shown to reduce the likelihood of dying in hospital, to reduce stress for patients and their relatives, and to increase patient concordant care[1]. Early family meetings (before hospital day 3) have been associated with reduced length of stay, fewer ventilator days, fewer deaths during ACLS, and earlier transition to comfort focused care [9].
Without these conversations, the default is to implement life-prolonging measures, which may ultimately be contrary to the patient’s and family’s preferences and unwanted. This creates a great opportunity for emergency room providers to engage in a conversation about goals of care which prioritize the values and priorities of older and terminally ill patients, which may include maximizing comfort and time at home [3].
A recent randomized controlled study conducted by Ouchi et al. published in JAMA in June of 2025 evaluated the impact emergency department led GOC conversations for older patients with seriously illness, facilitated by trained research RNs. 141 adults with serious illnesses (metastatic cancer, oxygen-dependent chronic obstructive lung disease, chronic kidney disease receiving dialysis, New York Heart Association class III or IV heart failure, or treating ED clinician “would not be surprised if the patient died in the next 12 months”) were randomly assigned to the GOC intervention or usual care. The primary outcome of interest was patient reported engagement in advanced care planning (ACP). At 3 months, there was a trend towards greater patient reported engagement in ACP among the intervention group that did not reach statistical significance (3.37 vs 3.37, p =0.07), but medical record documentation of end-of-life values was substantially higher in the intervention group (24.3% pts vs 9.9% pts, p = 0.008). The results of this study indicate that ED visits present an opportunity to have goals of care conversations a critical point in the patient’s illness trajectory that may set the tone for the rest of the patient’s hospitalization, ideally preventing unwanted interventions [4].
Best Approach to Goals of Care
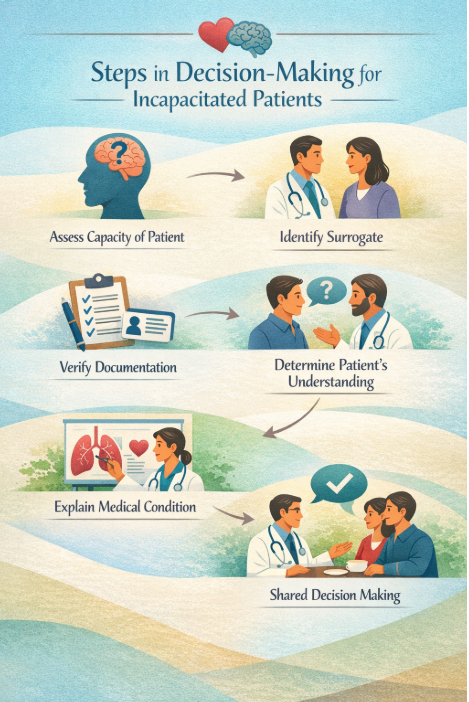
In the Emergency Department, we do not always have the luxury of time, especially when a patient’s condition is deteriorating rapidly and decisions have to be made quickly. This, however, does not mean we don’t have time for GOC conversations; rather, it means we need an efficient framework we can use at bedside to help guide GOC conversations when they matter most. Below we summarize a framework developed for the Emergency Department by EM physician and ethicist Walter Limestone,published in the Annals of Emergency Medicine.
Assess Patient’s Decision Making Capacity
Patients have the right to make decisions about their own bodies, and our job as providers is to respect their autonomy. Therefore, our first step is to determine if a patient is able to make decisions about their own care. Does the patient understand their condition, the proposed treatment options and the associated risks/benefits? Is the patient able to evaluate the consequence of each treatment choice? Is the patient consistent about their choice? If the answer is yes to all of the above, we can say with relative certainty that the patient has capacity to make their own decisions [5][12]
Identify a Surrogate
If a patient is unable to make a decision for themselves, the next step is to identify a surrogate decision maker. In some cases, patients will have appointed a health care proxy. However, it is important to note that the health proxy form must be available either digitally or in print in order for the health proxy to make decisions. If no health proxy has been appointed, a health care surrogate is based on the state's health care surrogacy laws. In the state of New York, the hierarchy of surrogacy is as follows: guardian, spouse/domestic partner, adult child >18 yrs old, parent, sibling older than 18, and finally a close friend. If a patient has multiple adult children, all children either need to opt in or out of medical decision making, and they need to reach a unanimous decision. The role of the health care surrogate is to make decisions for the patient based on the individual’s wishes and values and prioritize “what the patient would have wanted.” We as providers should discuss the patient’s condition and possible treatment options with the surrogate [5]. Social work can also be helpful in coordinating with family members.
Understand Patient’s Wishes through Aid of Advanced Directive
After a decision maker has been identified, the next step is to determine if the patient has an advanced directive - the health care proxy, a living will, or, in some states, a Medical Orders for Life Sustaining Treatment (MOLST) form. Each document provides information about a patient’s desires, but is slightly different. It is important to note that the power of attorney for health care does not exist in New York State.
When a patient has appointed a health care proxy, the patient declares a decision maker for when they do not have capacity and grants that decision maker the agency to determine medical care for the patient, including advancing/withdrawing care. Similarly, a living will details the patient’s specific wishes regarding interventions including intubation, resuscitation, and artificial nutrition. Of note, both a health care proxy and a living will only take effect once it has been determined that a patient does not have decision making capacity, and must be “activated” [5].
In the state of New York, an attending physician can determine if a patient does not have capacity. However, if medical care is to be withheld or withdrawn in accordance with the living will, another physician, nurse practitioner, or physician assistant must agree with this determination [6]. This must be documented in the medical record.
On the other hand, a patient does not need a capacity assessment in order for a MOLST to be active. A MOLST (also known as a Physician Orders for Life Sustaining Treatment or ‘POLST’) is a set of legally binding orders regarding resuscitation, ventilation, and other life saving measures that in the state of New York apply to both the pre-hospital and in-hospital setting and must be honored by EMS, nursing homes, hospices, and hospitals [7].
The above discussed documents provide significant insight into the patient's desires at the end of life regardless if they have formally taken effect and should be used to guide GOC conversations with family members or with the patient themselves [5].
Determine Patient’s/Surrogate’s Understanding of Medical Event
As Emergency Department providers, we are meeting patients and family members for the first time and must guide them through extremely difficult conversations. In order to have effective GOC conversations, it is important that we put ourselves in the shoes of our patients and their family members. Making end of life decisions for a loved one is extremely stressful as surrogates often do not have much time to make these decisions and process the information. Studies have demonstrated that surrogates for relatives in the ICU develop symptoms of post-traumatic stress disorder related to medical decision making [11].
Taking a family/patient centered approach to GOC conversations is essential in the Emergency Department, where we don’t always have the luxury of time to make decisions. This involves finding a quiet space for the conversation when possible (ideally not the hallway) and employing active communication strategies including maintaining eye contact, asking open-ended questions, and summarizing what the family has said. The “SPIKES” model is a widely used tool used in delivering difficult news, and is a six-step framework that involves preparing the setting, assessing the patient’s perception and understanding, inviting readiness to hear information, sharing knowledge clearly, responding with empathy, and summarizing next steps and care planning [10]. Additionally, allowing family members to watch resuscitation efforts may help families come to terms with the critical condition of their loved ones.[8].
Explain Physician’s Assessment of Medication Condition
After assessing what the patient/surrogate understands about the situation, we must share our understanding of the patient’s condition and possible treatment options taking into account the patient’s values and wishes. Use simple language that family members can understand. Giving our best estimate on the prognosis of the patient plays a critical role here, despite an exact prognosis being nearly impossible to provide in most instances. It can be helpful to provide families a range such as minutes to hours, hours to days, a few short weeks, acknowledging this is not absolute, and the patient's course may change. Family members often rely on prognosis to make a rapid decision about medical care [8].
Shared Decision Making
Ultimately we must guide the patient/surrogate through the decision making process. Part of this step involves making a treatment recommendation (e.g. continuing aggressive resuscitation vs comfort focused care) based on our understanding of the patient’s goals and preferences. It is helpful to have an understanding of the patient’s goals and values before making recommendations. Once you have a better understanding of the patient’s goals and values, you could make treatment recommendations based on those and avoid offering treatment options that would be contradictory. For example, if the family members know that the patient would never want to be dependent on a machine, then it would not make sense to offer CPR or intubation. As described above, the patient’s wishes and values should be at the heart of the discussions and decisions made. As the patient’s condition evolves and more information becomes available, the conversations and decisions about the goals of treatment should be continuously reassessed [8].
Challenges and limitations
As mentioned, GOC conversations can pose a challenge – particularly in the unique context of the emergency department. Patients may face intense emotions, be in critical condition, or be unable to communicate, and some may never have previously shared their care preferences. In addition, the fast-paced and often temporary environment of the emergency department makes it difficult for ER clinicians to engage in in-depth discussions such as GOC with time constraints being a limitation factor.
Clinician preparedness can also pose a challenge. According to Ouchi et al, it was noted that many emergency clinicians feel insufficiently trained or lack the confidence to facilitate GOC, which often leads to either skipping the conversation entirely or engaging in an overly rushed discussion. Systemic barriers also exist within the hospital system, as there is no standardized protocol or documentation to address GOC and adequately identify which patients would benefit from such conversations, or communication between inpatient and outpatient teams.This likely explains why this can be challenging in the ED, and why we as clinicians often defer them to the inpatient setting, leading to role uncertainty [1]. There are now communication programs like EMTalk that can specifically provide communication training for EM clinicians to help with this [13]. Rapid GOC discussion guides also exist that can be helpful in the emergency room [14].
Family dynamics can also complicate the matter. Goals-of-care conversations can involve multiple family members and surrogate decision-makers, who may hold conflicting views and be unprepared to make rapid decisions in the ED, especially during a moment of distress. In this context, health literacy and cultural norms can significantly influence these discussions both for patients and surrogate decision makers [1]. In these situations, seeking the help of social work, the chaplain, or palliative care can be helpful.
There is also a significant evidence gap that exists within the topic of GOC and how to best engage older or chronically ill patients in conversations, specifically in the context of the ED, which offers a unique opportunity for future research.
Conclusion
GOC conversations are essential to have in the Emergency Department as they are a core component to patient-centered medicine. However, these conversations often fall into the background in a setting that is frequently characterized by urgency, uncertainty and limited time such as the Emergency Room. Nevertheless, the ED is oftentimes the first point of contact for patients with serious or life-limiting medical conditions. Without GOC, physicians often default to life-prolonging measures which may conflict with patient wishes.
Emergency Department physicians are uniquely positioned in that they are able to have goals of care discussions during initial, pivotal moments of patient care. By using a structured, efficient framework—assessing decision-making capacity, identifying surrogates, reviewing advance directives, clarifying understanding, sharing prognosis, and engaging in shared decision-making, providers can ensure that all medical care performed honors patients’ and their families wishes. Even a brief or incomplete conversation can have a profound impact on patient care, reduce the amount of unwanted medical care, and ease patients’ and families emotional distress.
Despite challenges such as time constraints, clinician discomfort, systemic barriers, and complex family dynamics, research shows that it is feasible to have goals of care discussions in the ED and increased training in goals of care discussions will better prepare physicians to have these conversations. Ultimately, engaging in goals of care conversations in the ED honors patient autonomy and reframes resuscitation not as doing “everything,” but as honoring wishes of every individual patient. Even in moments of chaos, taking the time to ask and listen may be one of the most meaningful interventions we provide.
References:
Pajka, S. E., Hasdianda, M. A., George, N., Sudore, R., Schonberg, M. A., Bernstein, E., Tulsky, J. A., Block, S. D., & Ouchi, K. (2021). Feasibility of a Brief Intervention to Facilitate Advance Care Planning Conversations for Patients with Life-Limiting Illness in the Emergency Department. Journal of Palliative Medicine, 24(1), 31–39. https://doi.org/10.1089/jpm.2020.0067
Smith, A. K., McCarthy, E., Weber, E., Cenzer, I. S., Boscardin, J., Fisher, J., & Covinsky, K. (2012). Half Of Older Americans Seen In Emergency Department In Last Month Of Life; Most Admitted To Hospital, And Many Die There. Health Affairs, 31(6), 1277–1285. https://doi.org/10.1377/hlthaff.2011.0922
Ouchi, K., George, N., Schuur, J. D., Aaronson, E. L., Lindvall, C., Bernstein, E., Sudore, R. L., Schonberg, M. A., Block, S. D., & Tulsky, J. A. (2019). Goals-of-Care Conversations for Older Adults With Serious Illness in the Emergency Department: Challenges and Opportunities. Annals of Emergency Medicine, 74(2), 276–284. https://doi.org/10.1016/j.annemergmed.2019.01.003
Ouchi K, Block SD, Rentz DM, et al. Serious Illness Conversations in the Emergency Department for Older Adults With Advanced Illnesses: A Randomized Clinical Trial. JAMA Netw Open. 2025;8(6):e2516582. doi:10.1001/jamanetworkopen.2025.16582
Limehouse, W. E., Ramana Feeser, V., Bookman, K. J., & Derse, A. (2012). A Model for Emergency Department End-of-life Communications After Acute Devastating Events-Part I: Decision-making Capacity, Surrogates, and Advance Directives. Academic Emergency Medicine, 19(9), E1068–E1072. https://doi.org/10.1111/j.1553-2712.2012.01426.x
https://law.justia.com/codes/new-york/pbh/article-29-c/2983/
https://www.health.ny.gov/professionals in/ems/pdf/23-12.pdf
Limehouse, W. E., Ramana Feeser, V., Bookman, K. J., & Derse, A. (2012). A Model for Emergency Department in. Academic Emergency Medicine, 19(11), 1300–1308. https://doi.org/10.1111/acem.12018
Bhangu JK, Young BT, Posillico S, Ladhani HA, Zolin SJ, Claridge JA, Ho VP. Goals of Care Discussions for the Imminently Dying Trauma Patient. J Surg Res. 2020 Feb;246:269-273. doi: 10.1016/j.jss.2019.07.046. Epub 2019 Oct 12. PMID: 31614324; PMCID: PMC7006367.
Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311. doi:10.1634/theoncologist.5-4-302
Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med. 2005;171(9):987-994. doi:10.1164/rccm.200409-1295OC
Appelbaum PS. Assessment of Patients’ Competence to Consent to Treatment. New England Journal of Medicine. 2007;357(18):1834-1840. doi:https://doi.org/10.1056/nejmcp074045
Grudzen CR, Emlet LL, Kuntz J, Shreves A, Zimny E, Gang M, Schaulis M, Schmidt S, Isaacs E, Arnold R. EM Talk: communication skills training for emergency medicine patients with serious illness. BMJ Support Palliat Care. 2016 Jun;6(2):219-24. doi: 10.1136/bmjspcare-2015-000993. Epub 2016 Jan 12. PMID: 26762163.